WE’VE BEEN LIED TO ABOUT HYDROXYCHLOROQUINE
This is viewable in
Google Docs with footnotes.
Corrupt people in power compromise accepted principles of science to Mislead the World!
Introduction: This is a layman’s look, about 12 hours of work compiling, sorting and analyzing reports for and studies against the effectiveness of HCQ. All research was done looking for core data as a basis. There are very few opinions shared (other than mine) that aren’t related to observed data. I also have no background in investigative reporting. If my research is valid, it points to either an inept job by all of mainstream media or a bias against HCQ and it’s promoters that resulted in countless deaths. Starting on page 15 are pastes from websites that give sources for much of the information used as a basis for the below analysis. Links are in footnotes.
CONTENTS
ANALYSIS
Spoiler
Summary
Claims of near zero deaths with use of Hydroxychloroquine(HCQ)
Need for control groups and randomized trials:
Control groups and randomized trials
Study flaws
Comparing death rates in the UK Trial to other studies
FDA after approving HCQ now calls it dangerous!
Patients in Study were very sick and were given probably toxic doses of HCQ.
FDA Cherry-Picks data
The WHO summarizes the studies differently.
A couple of reports to consider
American Frontline Doctors White Paper
A Leading Scientist About the Controversy
Ramp up early outpatient treatment of symptoms
Evidence of HCQ Conspiracy
Evidence for Effectiveness
Evidence for Ineffectiveness
Negative side effects
TIMELINE
Compromise on almost every level.
EVIDENCE
ANALYSIS
SPOILER: If your conclusion is the same as mine after reading this, it should send chills down your spine. Either there’s a statistically improbable conclusion that Federal and State health agencies including the FDA along with reputable journals and studies run by Doctors and professionals all made huge mistakes analyzing data, or something insidious and dangerous has gone on. In any event, it may have led to up to 100,000 US deaths and multiples of that worldwide.
SUMMARY: Many doctors and hospitals reported amazing results of minimal or no deaths from Covid-19 when EARLY in treatment, Hydroxychloroquine along with Azithromycin and/or Zinc were administered. Soon after, many studies were done to seemingly contradict the encouraging results. However, none of the studies mirrored what was found to be effective. They either administered late in treatment, gave what is believed to be toxic doses, or didn’t include the other effective drugs. Agencies went against their own standards in interpreting data to come to their conclusions.
Claims of near zero deaths with use of Hydroxychloroquine(HCQ) Starting in late March, 2020, some Doctors and hospitals citing thousands of success stories made amazing claims of zero deaths in many cases when they, early in the progression of Covid-19 caused illness, used a cocktail of up to three drugs/minerals: Hydroxychloroquine, Azithromycin (AZ), and Zinc. Their claims were based on mostly anecdotal data and without control groups. However, with mounting deaths in the “control group” of the rest of the world, their professional observations were both compelling and encouraging.
Need for control groups and randomized trials: Clearly large randomized trials needed to be completed to confirm or reject the anecdotal evidence. Since the anecdotal evidence was widespread both in the number of doctors and number of patients (well over 10,000), and extremely successful in treatment, studies needed to replicate similar treatment programs. However, none did so.
Control groups and randomized trials: Studies with control groups were completed around that time and soon thereafter concluding that Hydroxychloroquine wasn’t effective in hospital settings with sick patients. Those studies seem to correctly conclude that HQC alone may be ineffective at treating mid to late term cases. They are however flawed if attempting to conclude that HCQ is simply “ineffective” if given early and/or with other drugs. The studies have additional flaws.
Study flaws:
A small percentage of studies in addition to HCQ, included an additional component. For example, HCQ was given with Azithromycin but not given early. I couldn’t find any studies that included at least 2 of the components that the proponents said resulted in lower deaths and less serious sickness.
Given early in treatment
Azithromycin (suggested by some Doctors)
Zinc (suggested by some Doctors)
In more than one study, (including the large randomized trial) patients were given well beyond the maximum recommended dosage resulting in what is believed by some to be death by poisoning.
The number of people given HCQ in five controlled studies were 15, 31, 107, 150, 241 (10% death rate) and 1561 (25%+ death rate), only two “large” trials.
Two of the studies had nothing to do with treatment but rather prevention.
Two others tested what seems to have been very sick patients with death rates in both HCQ and control groups. The two “large” studies had 10% death rates (241 given HCQ) and another 25% (418/1561 given HCQ died, 788/3155 in control group died).
The total of patients given HCQ (not along with Azithromycin and Zinc) in other than the one study where 25% died is 302. Compare that to the documented over 4100 patients and the patients of over 2500 physicians who had success with it citing ZERO or near zero deaths.
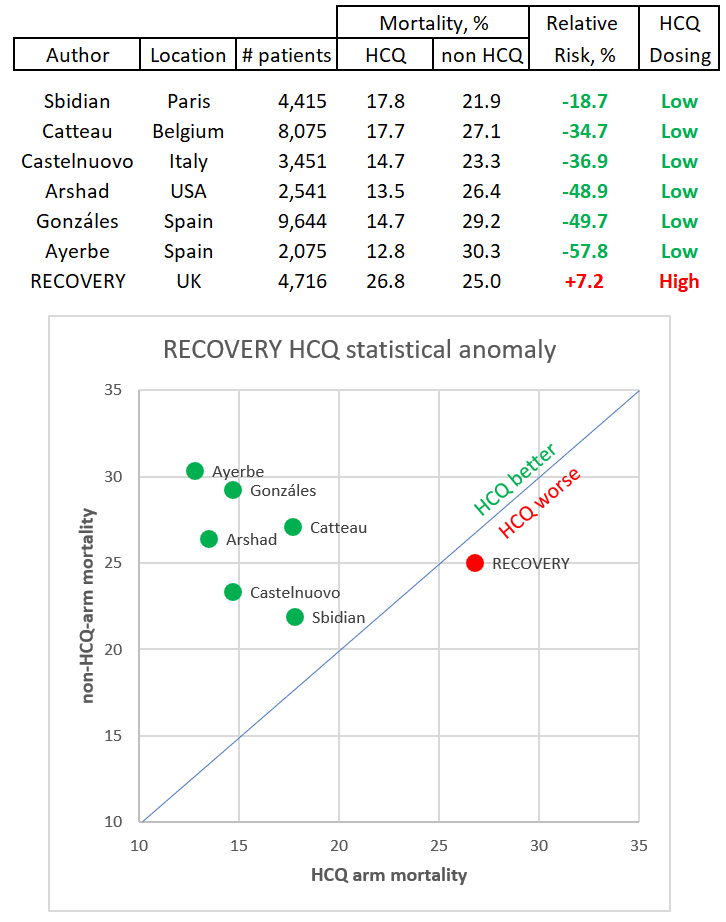
Comparing Death Rates in the UK (largest) Trial to other studies.
I have not confirmed the veracity of the above chart. If true, it confirms the views of many Doctors that the high dose of HCQ in the UK trial (the large randomized trial used by the FDA and others to indicate that HCQ was ineffective) contributed to increased deaths. In any event deaths in both groups indicated patients were very sick at the onset of treatment. https://cvpandemicinvestigation.com/hydroxychloroquine-hcq-evidence-of-conspiracy-that-killed-over-100k-americans/
FDA after approving HCQ now calls it dangerous!
Patients in Study were very sick and were given probably toxic doses of HCQ. Some in leadership at the FDA and two highly regarded medical journals went against their own standards for evidence and publicly concluded that HCQ wasn’t effective. The Lancet and New England Journal of Medicine retracted their reports.
The FDA touted a large randomized trial as their basis for revoking emergency use of HCQ. It doesn’t take medical experience for someone to question the conclusion that HCQ is simply ineffective based on that trial. In fact, after writing this, I read the comments that noted similar concerns. The death rate for the control and HCQ group was over 25% indicating these were very sick patients. Those given HCQ were given well over the highest recommended dose on day 1 of treatment. How can the FDA make a decision for early use of HCQ along with Azithromycin and Zinc based on a trial that only gave HCQ in possibly toxic quantities late in treatment?
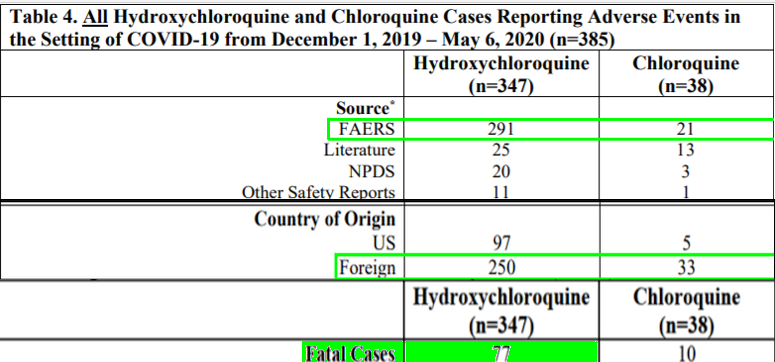
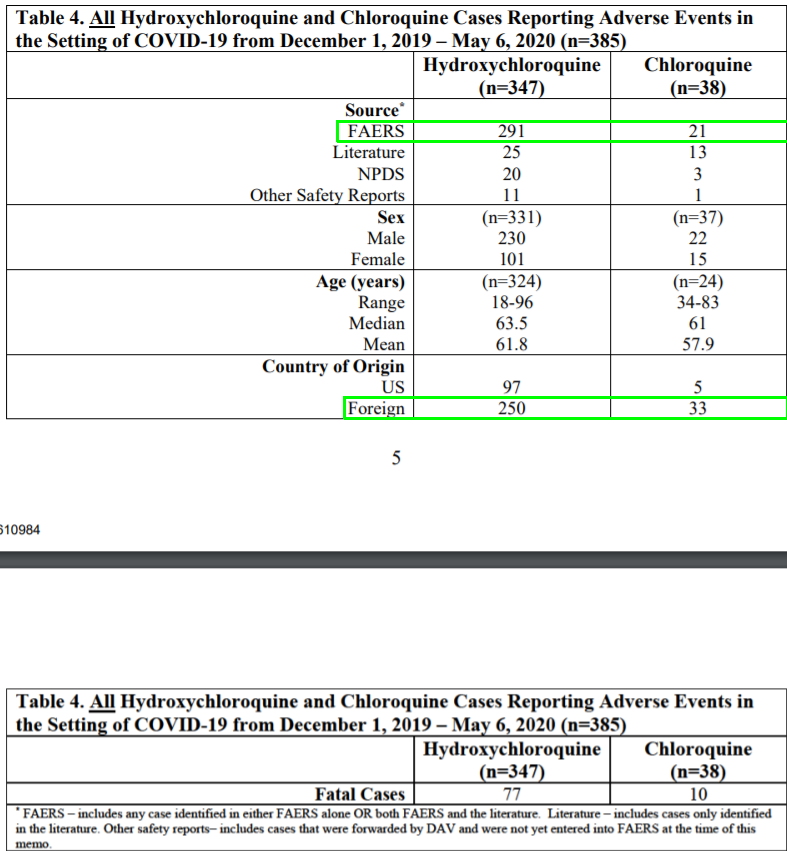
The most unbelievable part yet is the FDA calling HCQ dangerous. The FDA concluded that HCQ “in light of ongoing serious cardiac adverse events and other potential serious side effects, the known and potential benefits of chloroquine and hydroxychloroquine no longer outweigh the known and potential risks for the authorized use.” This is a FDA approved drug used for over 60 years, billions of doses! Now it’s dangerous? They seemed to have switched to another study to come to this conclusion: “Notably, 84% of hydroxychloroquine and chloroquine cases reporting a serious cardiac adverse event” Over 83% of that data (291/347) came from FAERS. At the bottom of the same page: “FAERS data cannot be used to calculate the incidence of an adverse event or medication error in the U.S. population. Now if this doesn’t make you wonder, then consider that in the “LARGE RANDOMIZED TRIAL- UK Study” where 1561 patients were given HCQ and where 25% of the patients died, the conclusion was “There was no excess of new major cardiac arrhythmia.” So, they cherry picked (See below) from two groups of seemingly conflicting data. The high percentage of deaths indicates the data didn’t come from studies or situations comparable to the successful anecdotal results (Early treatment). And yet the FDA used this to officially reject the emergency use of HCQ. This isn’t some High School debater hoping to pull one off (wouldn’t even work there). It’s the FDA!!!
FDA Cherry-Picks data
The information on this page are from a single FDA report.
Results (UK Study )1561 patients randomly allocated to receive hydroxychloroquine were compared with 3155 patients concurrently allocated to usual care. Overall, 418 (26.8%) patients allocated hydroxychloroquine and 788 (25.0%) patients allocated usual care died within 28 days (rate ratio 1.09; 95% confidence interval [CI] 0.96 to 1.23; P=0.18). Consistent results were seen in all pre-specified subgroups of patients. Patients allocated to hydroxychloroquine were less likely to be discharged from hospital alive within 28 days (60.3% vs. 62.8%; rate ratio 0.92; 95% CI 0.85-0.99) and those not on invasive mechanical ventilation at baseline were more likely to reach the composite endpoint of invasive mechanical ventilation or death (29.8% vs. 26.5%; risk ratio 1.12; 95% CI 1.01-1.25). There was no excess of new major cardiac arrhythmia.
In addition, there are the thousands of cases of success with NO DEATHS from Covid OR Cardiac issues. They had access to a study in France of 1061 patients who took HCQ and AZ. “No cardiac toxicity was observed.”
The WHO summarizes the studies differently.
“Current data shows that this drug does not reduce deaths among hospitalised COVID-19 patients, nor help people with moderate disease.”
“More decisive research is needed to assess its value in patients with mild disease or as pre- or post-exposure prophylaxis in patients exposed to COVID-19.
Studies of seriously ill hospitalized patients were stopped because data didn’t show it reduced mortality.”
The “it” here is HCQ alone. One study did show it to be effective even later in treatment when combined with the other drugs. So, why not say, “HCQ alone?”
ARTICLES WORTH A READ
AMERICAN FRONTLINE DOCTORS
I skimmed this white paper a while back and have not read it since. I want to start from scratch when investigating something. I’ll link it here because it’s far better at presenting the pro argument than what I’m sharing below. https://www.americasfrontlinedoctors.com/wp-content/uploads/2020/09/White-Paper-on-HCQ-2020.2.pdf
A LEADING SCIENTIST ABOUT THE CONTROVERSY
These studies indicate that some scientists either forgot how “science” is done or that there is a huge effort to disprove, whatever it takes, that HCQ works.How can someone or even Councils and Academies of Medicine cite such studies as the “science” of their decisions? How can that be?
EVIDENCE OF HCQ CONSPIRACY
I skimmed through this webpage that discusses the success of HCQ, overdosing, media cherry picking of information. It’s worth a look at for additional information. https://cvpandemicinvestigation.com/hydroxychloroquine-hcq-evidence-of-conspiracy-that-killed-over-100k-americans/
Evidence for effectiveness.
(The below aren’t studies. However they are the conclusions of observed data from Doctors. This list is supported in the Evidence Section below along with sources)
Dr. Brian Tyson 1700 patients 0 deaths
Dr. Hernandez: Lower hospitalizations and lower mortality
Dr. Risch 7 studies showed significant benefit
American Association of American Physicians 2333 patients, helped 91% recover
Dr. Marcus Zervos: Mortality was 13.5% with vs 26.4% without only using HCQ.
Dr. Cardillo (Urgent Care) Very ill patients recovered in 8-12 hours. (Included Zinc).
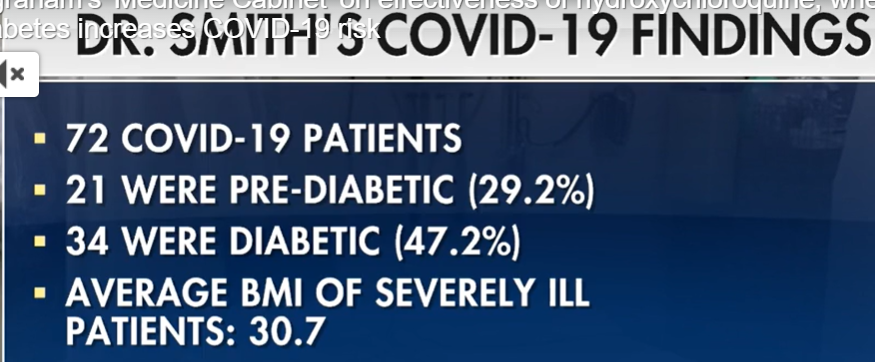
Dr. Steven Smith: 72 patients, no intubation or death
Dr. Stella Immanuel 350 patients, no deaths
50% of 1337 Physicians used it and 40% found it effective.
6227 Physicians in 30 countries 37% said most effective.
These are controlled trials of unknown quality.
China: 48 patients out of 500 had 19% fatalities compared with 47%
IHU France: 1061 Patients given HCQ and AZ with positive results. Mar 3-Apr 9, 2020
As a prophylactic
“Consumption of four or more maintenance doses of HCQ was associated with a significant decline in the odds of getting infected” June 5
Study
Henry Ford
NYU Grossman School of Medicine: Zinc sulfate added to hydroxychloroquine and azithromycin may improve outcomes among hospitalized patients. The decrease in mortality or transition to hospice was most striking when considering only patients who were not admitted to the ICU
“Evidence” for ineffectiveness.
Study 1,(HCQ only, HIGH DOSE, LATE) NCT04381936 the UK Study RECOVERY said HCQ was ineffective. However they had a very high death rate for both groups, 25%. Right away, having observed that the proponents noted that the cocktail needed to be given early in treatment, the high death rate indicated that this group were either more ill and/or given it later. Later while compiling information, I read this, “But some scientists say they want to see the full data before making up their minds. About one in four patients died in both arms of the study, Kremsner notes—a very high rate, suggesting they were gravely ill when treatment started.”
Study 2, (HCQ only, Prophylactic) NCT4308668 University of Minnesota (Prong 1 of Study 5) No official results posted as of 4/5/21 This study tested whether HCQ kept people from getting Covid. Patients were only administered HCQ. 1821 exposed to Covid, 86% were healthcare workers who spent over 10 minutes with 6 feet of an infected person with no face mask or shield.(Side note: Only 15% got infected!) Total infected group size is 107, median age of 41. HCQ group 11.8% illness, non HCQ 14.3%. “This randomized trial did not demonstrate a significant benefit of hydroxychloroquine as postexposure prophylaxis for Covid-19” The title to this report could have accurately read, “HCQ resulted in a 21% decrease in infections.” (14.3%-11.8%)/11.8%
Study 3 (HCQ only, HIGH DOSE) ChiCTR2000029868 11 to 29 February 2020 of 2300 people (two pronged, preventing infection and effectiveness as a treatment). It seems to end up only studying 150 people who actually showed symptoms and were 18 and over which could have included very low risk groups. Results still not posted from May, 2020 study. They also administered “1200 mg daily for three days followed by 800 mg daily..two or three weeks” In 2 weeks, that’s 12.4 grams, considered toxic. (See more on this under adverse side effects below).
Study 4 (HCQ only, LATE) NCT04332991 JAMA resulted in a 10% death rate for both groups, better than Study 1, suggesting people weren’t as sick. But still, they were quite sick. “20.1% in the intensive care unit; 46.8% receiving supplemental oxygen without positive pressure; 11.5% receiving noninvasive ventilation or nasal high-flow oxygen; and 6.7% receiving invasive mechanical ventilation or extracorporeal membrane oxygenation)” I searched all 3 supplements and couldn’t find out if there’s an overlap in the percentages If not 85.1% of the patients were already sick enough to be on oxygen. If there’s an overlap, then 65% are. In any event, these are most probably not being given HCQ EARLY and again, they weren’t given the cocktail touted to be effective.
Study 5 (HCQ only)NCT4308668 University of Minnesota (Prong 2 of Study 2) No official results posted as of 4/5/21 423 patients. 341 had infection or exposure. 236 enrolled within 1 day of symptoms. At 14 days 24% (49/201) of HCQ vs. 30% (59/194) of placebo still had symptoms. With HCQ 4 hospitalizations vs. 10 (2 non-Covid) If these 2 were for completely unrelated health issues or(car accident, etc., the removal of this data is valid. Otherwise death from Covid-19 is currently determined by death WITH Covid. One death in each group with HCQ death nonhospitalized. “Conclusion: Hydroxychloroquine did not substantially reduce symptom severity in outpatients with early, mild COVID-19.” I’m confused at this conclusion. With HCQ 4/201, 2% hospitalization vs. at least 8/194, over 4% hospitalization, it seems HCQ reduced hospitalizations by double! Of course this is a very small sample but the conclusion it didn’t substantially reduce severity can’t be substantiated with this study. It’s not clear how severe the hospitalization cases were. In any event, the title to this report could have accurately read, “HCQ alone results in over a 50% decrease in hospitalizations.” REBUTTAL TO STUDY 5. Scroll to the bottom to read comments from Doctors and researchers about flaws in this study.
Excerpts: Folic acid is effective against Covid so it isn’t a good placebo.” “ “authors seem to disregard their own HCQ positive results found when patients taking >75% of the tablets are considered”
Negative side effects
"Common sense tells us this, that a medication safely used for 65 years by hundreds of millions of people in tens of billions of doses worldwide, given to adults, children, pregnant women and nursing mothers, must be safe when used in the initial viral-replication phase of an illness that is similar at that point to colds or flu," he said.
Out of 1561 (UK Study) in a controlled study, “There was no excess of new major cardiac arrhythmia.”
University of Michigan Study where 414 given HCQ: “but no serious adverse reactions were reported.”
JAMA Study: They administered “1200 mg daily for three days followed by 800 mg daily..two or three weeks” In 2 weeks, that’s 12.4 grams, considered toxic. Still, out of 75, “Two hydroxychloroquine recipients reported serious adverse events.
The FDA concluded on May 19,2020 that HCQ had significant negative side effects. I’m very confused by the data which isn’t directly sourced. Out of 341 Cases, data from 291 came from FAERS. In the Appendix, they discuss why this is the case: “FAERS data cannot be used to calculate the incidence of an adverse event or medication error in the U.S. population.” AND “If a potential safety concern is identified in FAERS, further evaluation is performed.” I was unable to find any of this data in FAERS.
American Journal of Medicine August,2020 “HCQ was approved by the US Food and Drug Administration in 1955, has been used by hundreds of millions of people worldwide since then, is sold over the counter in many countries, and has a well-characterized safety profile that should not raise undue alarm”
Some of the controlled studies cite this safe drug as now dangerous. As noted above, one study gave patients 2 ½ times the recommended dose which doctors indicate would be poisonous. (Opinion report) Below from WHO study in 1979.
TIMELINE
February 25 Chinese pilot study 15 patients given HCQ without better results.
March 19: French study of 30 patients indicates positive results for HCQ and AZ.
March 21: Trump Tweeted “HYDROXYCHLOROQUINE & AZITHROMYCIN, taken together, have a real chance to be one of the biggest game changers in the history of medicine.
March 28: Some governors ban or restrict Doctors from prescribing HCQ.
March 28, FDA authorized the emergency use of hydroxychloroquine and chloroquine supplied from the Strategic National Stockpile to treat adults and adolescents who weigh 50 kg or more and are hospitalized with COVID-19 for whom a clinical trial is not available, or participation is not feasible.
March 31: Dr. Steven Smith reports 72 Patients, 0 Deaths
April 13, 2020, the Division of Anti-infective (DAI) products opened a priority Tracked Safety Issue (TSI) 2150 to assess the risk of cardiac toxicity with hydroxychloroquine and chloroquine with or without azithromycin when used for the treatment of COVID-19 caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.
April 21, 2020 VA Study shows HCQ causes increased deaths. Mainstream Media reports.
April 23, 2020 Laura Ingram along with Dr. Martenson exposes the fact that the VA study is a “garbage study” and is being used to push a political narrative. Rick’s Note!
April 24, FDA issued a Drug Safety Communication (DSC) cautioning against the use of hydroxychloroquine or chloroquine for COVID-19 outside of the hospital setting or a clinical trial due to risk of arrhythmias. The DSC described reports of serious cardiac events, including QT prolongation, in patients receiving hydroxychloroquine or chloroquine, often in combination with azithromycin and other QT prolonging medicines, for the prevention or treatment of COVID-19.1
April 26 regarding VA Study: VA Secretary Robert Wilkie briefly mentioned the study in an interview with MSNBC last week, downplaying its results."That's an observational study," he said. "It's not a clinical study. It was done on a small number of veterans — sadly, those of whom were in the last stages of life, and the drug was given to them. And I have to also say that we know the drug has been working on middle-age and younger veterans."
May 6, DAV consulted the Office of Surveillance and Epidemiology (OSE) to review clinical trials, observational studies, and postmarketing surveillance data published or available after the March 28, 2020 EUA for hydroxychloroquine and chloroquine in the setting of COVID19 and comment on implications of these data regarding known and potential risks of the authorized use. DPV’s analysis focused on the available safety data reporting the use of hydroxychloroquine or chloroquine for the treatment or prevention of COVID-19 in any setting.
May 22: Lancet publishes article denouncing HCQ
May 27: American Journal of Epidemiology recommends HCQ.
May 29: Lancet study challenged
June 3 Minnesota Study of 821 people (107 with Covid) showed HCQ didn’t prevent Covid. Median age 41. No serious side effects. And they were given 2.5 Max dosage day 1 and max for 4 days after.
June 4: Lancet retracts article due to issues with source information.
June 5: UK Study: Large trial of 1561 patients given HCQ finds it ineffective. Death rate for both groups was 25%. HCQ group was given 2000mg in 12 hours, 5 times normal dosage and over 3 times maximum dosage for 24 hours!
June 15: FDA Revokes Emergency Use Authorization: This action was taken following a rigorous assessment by scientists in our Center for Drug Evaluation and Research,” But they still say, “FDA approved products may be prescribed by physicians for off-label uses if they determine it is appropriate for treating their patients, including during COVID.” They base this on a large randomized trial and other scientific data. The only trials I’m able to find are the June 3rd and June 5th ones. The FDA also used significant data from FAERS even though they note: “ FAERS data cannot be used to calculate the incidence of an adverse event or medication error in the U.S. population” 291 out of 347 reports of adverse reactions to HCQ came from FAERS.
June 15: Still not published as of 4/2021 study of 150 people showed HCQ ineffective.
June 20: NIH Halts HCQ Study, No Good, No Harm citing PETAL ORCHID
July 1 Update: A summary of the FDA review of safety issues with the use of hydroxychloroquine and chloroquine to treat hospitalized patients with COVID-19 is now available. This includes reports of serious heart rhythm problems and other safety issues, including blood and lymph system disorders, kidney injuries, and liver problems and failure. This seems to come from a study where 291/347 patient information came from FAERS.
July 2: Henry Ford Study indicates HCQ is effective.
July 27 American Frontline Doctors calls HCQ studies “fake science.” Wrong patients (too sick) and poisoning with HCQ.
Compromise on almost every level.
Organizations, some normally trustworthy, cite flawed studies as reason for ineffectiveness or present Hydroxychloroquine as ineffective but hidden in the text clarifies the position is in relation to sick hospitalized patients, not early treatment of mild conditions. WebMD, NIH, FDA “We made this determination based on recent results from a large, randomized clinical trial” Science Tech Daily Headline New Research Finds Hydroxychloroquine Is Not a Possible Defense Against COVID-19 Body: “Treatment with HCQ early in the disease or for mild cases is still under review.”
Lancet a very highly respected medical journal, retracted its report after not being able to confirm data from a suspicious source, Surgisphere. (I haven’t studied this. A post along with what looks like an informative video. “The science editor for this 6 person company is Thomas Koenigsberger who died in 2018. The other science editor is a digital artist whose photo was taken from her fineartamerica page. Also there appears to be no data scientists on the staff of the company in charge of collecting the data.”
The Mainstream Media The bias was incredibly one sided seemingly in order to affect Trump's image as he supported the use of HCQ. Trump’s name is used repeatedly across multitudes of news sources with the story of HCQ not being effective and/or being dangerous.
Censorship of America Frontline Doctors from Facebook and YouTube
Data possibly suggesting the ineffectiveness of HCQ: I haven’t and don’t plan to research why Brazil who has embraced the use of HCQ now has increasing deaths. Maybe it isn’t being used early, widely or with the rest of the cocktail.
BELOW ARE QUOTES FROM WEBSITES OF EACH SIDE OF THIS ISSUE. The below supports what is above this line and is provided as source material.
PRO USE OF HYDROXYCHLOROQUINE:
HIGH SUCCESS RATE
Dr. Brian Tyson from Southern California is one of the latest doctors to grant an interview talking about his experience in treating over 1700 COVID patients using hydroxychloroquine. None of his patients have died, and only one had to be admitted to the hospital.
Risch also said that in all seven studies examining the early use of the drug in high-risk outpatients have shown a "significant benefit."
The latest Sermo survey, which was taken between April 6 and April 9, found that of the 1,337 physicians surveyed who have treated patients with coronavirus, 50 percent have used Hydroxychloroquine or Chloroquine, which is the second most behind Azithromycin or similar antibiotics (58 percent.)
However, when asked about the effectiveness of treatments, 46 percent of respondents answered that "plasma from patients who have recovered from COVID-19" was either "effective" or "extremely effective," compared with 40 percent for Hydroxychloroquine or Chloroquine.
"We've used it on several hundred patients of ours and so far it's pretty good," Hernandez said. "We have lower hospitalizations and lower mortality."
The Association of American Physicians and Surgeons wrote a letter to Arizona Governor Doug Ducey urging wider use of hydroxychloroquine to treat covid
They claim that data on 2,333 coronavirus patients reveals the drug helped 91% of patients recover
In-hospital mortality was 18.1 percent overall; 13.5 percent with just hydroxychloroquine, 22.4 percent with azithromycin alone, and 26.4 percent with neither drug. "Prospective trials are needed" for further review, the researchers note, even as they concluded: "In this multi-hospital assessment, when controlling for COVID-19 risk factors, treatment with hydroxychloroquine alone and in combination with azithromycin was associated with reduction in COVID-19 associated mortality."
"Our results do differ from some other studies," Dr. Marcus Zervos, who heads the hospital's infectious diseases unit, said at a news conference. "What we think was important in ours ... is that patients were treated early. For hydroxychloroquine to have a benefit, it needs to begin before the patients begin to suffer some of the severe immune reactions that patients can have with COVID."
In this multi-hospital assessment, when controlling for COVID-19 risk factors, treatment with hydroxychloroquine alone and in combination with azithromycin was associated with reduction in COVID-19 associated mortality. Prospective trials are needed to examine this impact.
"Every patient I've prescribed it to has been very, very ill and within 8 to 12 hours, they were basically symptom-free," Cardillo told Eyewitness News. "So clinically I am seeing a resolution."
Cardillo is the CEO of Mend Urgent Care, which has locations in Sherman Oaks, Van Nuys and Burbank.
He said he has found it only works if combined with zinc. The drug, he said, opens a channel for the zinc to enter the cell and block virus replication.
Dr. Stephen Smith, founder of The Smith Center for Infectious Diseases and Urban Health, said on “The Ingraham Angle” on Wednesday night that he is optimistic about the use of antimalarial medications and antibiotics to treat COVID-19 patients, calling it “a game-changer.”
Smith, who is treating 72 COVID-19 patients, said that he has been treating "everybody with hydroxychloroquine and azithromycin [an antibiotic]. We’ve been doing so for a while.”
He pointed out that not a single COVID-19 patient of his that has been on the hydroxychloroquine and azithromycin regimen for five days or more has had to be intubated.
An international poll of thousands of doctors rated the Trump-touted anti-malaria drug hydroxychloroquine the best treatment for the novel coronavirus.
Of the 6,227 physicians surveyed in 30 countries, 37 percent rated hydroxychloroquine the “most effective therapy” for combating the potentially deadly illness, according to the results released Thursday.
This is what I will say to all those studies — they had high doses, they were given the wrong patients — I would call them fake science. Any study that says hydroxychloroquine doesn’t work is fake science. And I want them to show me how it doesn’t work. How is it going to work for 350 patients for me, and they are all alive, and then somebody says it doesn’t work? Guys, all them studies: fake science.
Evidence about use of HCQ alone, or of HCQ + AZ in inpatients, is irrelevant with regard to the efficacy of HCQ + AZ in early high-risk outpatient disease. Five studies, including 2 controlled clinical trials, have demonstrated significant major outpatient treatment efficacy.
LIMITED NEGATIVE SIDE EFFECTS.
Meanwhile, Harvey Risch, another of the expert witnesses from Yale University, said in his testimony that he found hydroxychloroquine in early use among high risk outpatients to be "exceedingly safe."
"Common sense tells us this, that a medication safely used for 65 years by hundreds of millions of people in tens of billions of doses worldwide, given to adults, children, pregnant women and nursing mothers, must be safe when used in the initial viral-replication phase of an illness that is similar at that point to colds or flu," he said.
There was no excess of new major cardiac arrhythmia.
CON USE OF HYDROXYCHLOROQUINE
INEFFECTIVE SO WASTE OF TIME AND RESOURCES.
Results from a controlled clinical trial from China on the use of hydroxy chloroquine as a treatment for Covid-19 have shown no significant differences in health outcomes between the control group and patients who received the experimental drug.
Thirty patients hospitalized for Covid-19 participated in the trial. Fifteen were treated with 400mg of chloroquine for five days and fifteen received standard supportive care
UK Study 1561 patients randomly allocated to receive hydroxychloroquine were compared with 3155 patients concurrently allocated to usual care. Overall, 418 (26.8%) patients allocated hydroxychloroquine and 788 (25.0%) patients allocated usual care died within 28 days (rate ratio 1.09; 95% confidence interval [CI] 0.96 to 1.23; P=0.18). Consistent results were seen in all pre-specified subgroups of patients. Patients allocated to hydroxychloroquine were less likely to be discharged from hospital alive within 28 days (60.3% vs. 62.8%; rate ratio 0.92; 95% CI 0.85-0.99) and those not on invasive mechanical ventilation at baseline were more likely to reach the composite endpoint of invasive mechanical ventilation or death (29.8% vs. 26.5%; risk ratio 1.12; 95% CI 1.01-1.25). There was no excess of new major cardiac arrhythmia.
Patients allocated to hydroxychloroquine sulfate (200mg tablet containing 155mg base equivalent) received a loading dose of 4 tablets (800 mg) at zero and 6 hours, followed by 2 tablets (400 mg) starting at 12 hours after the initial dose
The maximum recommended dosage is 600, normally 400mg. In the first 12 hours, these patients were given 800+800+400=2000mg, 2400mg in the first 24 hours.
Conclusions In patients hospitalized with COVID-19, hydroxychloroquine was not associated with reductions in 28-day mortality but was associated with an increased length of hospital stay and increased risk of progressing to invasive mechanical ventilation or death.
LANCET REPORT: Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis RETRACTED!
The Lancet paper was what brought Surgisphere under scrutiny as it focused on the safety and effectiveness of the malaria drug hydroxychloroquine for COVID-19, which had already become a political and scientific controversy, in large part because of Trump’s embrace of the drug. As soon as the study was published, it came under attack by clinicians, as well as experts in biostatistics and medical ethics who questioned how Surgisphere, a tiny company without much publishing experience in big data analysis, could have collected and analyzed tens of thousands of patient records from hundreds of hospitals—particularly given the complexities of navigating patient confidentiality agreements.
Leigh Turner, a bioethicist at the University of Minnesota, Twin Cities, calls the retractions “unnerving and disturbing.” He said the Surgisphere case raises a bigger question about how much access to key data each author and each journal should require. “The less access they have, the greater the chances that there will be errors, data fabrication, or outright fraud.”
However, the failure to resolve such basic concerns about the data during the course of normal peer review raises serious questions about the standard of editing at the Lancet and NEJM — ostensibly two of the world’s most prestigious medical journals.
ORCHID STUDY: By June, the study was stopped because interim results showed the drug neither caused harm nor improved patient outcomes. The trial had enrolled 479 of the expected 510 patients.
JAMA STUDY: Researchers led by Dr. Wesley Self of Vanderbilt University have now completed a final analysis of the study data. Their findings were published in JAMA on November 9, 2020.
The 479 patients who enrolled were randomly assigned to receive hydroxychloroquine or a placebo. The trial included 290 Latino and Black participants. The median patient age was 57. They received 10 doses of either hydroxychloroquine or a placebo over five days (400 mg twice daily on the first day, then 200 mg twice daily for the following four days).
Researchers assessed each patient’s condition 14 days after being assigned to a treatment group. They used a seven-category scale ranging from one (death) to seven (discharged from the hospital and able to perform normal activities). The results showed no significant difference between the hydroxychloroquine and placebo groups.
Results Among 479 patients who were randomized (median age, 57 years; 44.3% female; 37.2% Hispanic/Latinx; 23.4% Black; 20.1% in the intensive care unit; 46.8% receiving supplemental oxygen without positive pressure; 11.5% receiving noninvasive ventilation or nasal high-flow oxygen; and 6.7% receiving invasive mechanical ventilation or extracorporeal membrane oxygenation), 433 (90.4%) completed the primary outcome assessment at 14 days and the remainder had clinical status imputed. The median duration of symptoms prior to randomization was 5 days (interquartile range [IQR], 3 to 7 days). Clinical status on the ordinal outcome scale at 14 days did not significantly differ between the hydroxychloroquine and placebo groups (median [IQR] score, 6 [4-7] vs 6 [4-7]; aOR, 1.02 [95% CI, 0.73 to 1.42]). None of the 12 secondary outcomes were significantly different between groups. At 28 days after randomization, 25 of 241 patients (10.4%) in the hydroxychloroquine group and 25 of 236 (10.6%) in the placebo group had died (absolute difference, −0.2% [95% CI, −5.7% to 5.3%]; aOR, 1.07 [95% CI, 0.54 to 2.09]).
David Boulware of the University of Minnesota, Twin Cities, and colleagues published the results of the largest study to date of this strategy, called postexposure prophylaxis (PEP). The researchers sent either hydroxychloroquine or a placebo by mail to 821 people who had been in close contact with a COVID-19 patient for more than 10 minutes without proper protection. They reported in The New England Journal of Medicine that 12% of the people who took the drug went on to develop COVID-19 symptoms, versus 14% in a placebo group, a difference that was not statistically significant.
We enrolled 821 asymptomatic participants. Overall, 87.6% of the participants (719 of 821) reported a high-risk exposure to a confirmed Covid-19 contact. The incidence of new illness compatible with Covid-19 did not differ significantly between participants receiving hydroxychloroquine (49 of 414 [11.8%]) and those receiving placebo (58 of 407 [14.3%]);
Empirical data for the efficacy of HCQ in hospitalized Covid-19 patients became available after the start of this study; HCQ administration did not result in a significantly higher PCR negative conversion in a RCT including 150 patients and there was no reduction in the risk of death/intubation in two large observational studies.
Study 1 -We investigated the efficacy and safety of HCQ to prevent secondary SARS-CoV-2 infection and Covid-19 disease in contacts exposed to a PCR-positive Covid-19 case during.
Study 2- We also conducted a study to test the hypothesis that HCQ treatment would be more efficacious than no-treatment for patients with mild Covid-19.
Initially, the protocol included the use of combined treatment with a HIV protease inhibidor (cobicistat-boosted darunavir) for cases (study 2), but it was adapted to HCQ alone after the recommendation of the pharmaceutical company not to use DRVc for the treatment of Covid-19 due to lack of activity in-vitro.
FDA REVOKES USE: We now believe that the suggested dosing regimens for CQ and HCQ as detailed in the Fact Sheets are unlikely to produce an antiviral effect.
• Earlier observations of decreased viral shedding with HCQ or CQ treatment have not been consistently replicated and recent data from a randomized controlled trial assessing probability of negative conversion showed no difference between HCQ and standard of care alone.
• Current U.S. treatment guidelines do not recommend the use of CQ or HCQ in hospitalized patients with COVID-19 outside of a clinical trial, and the NIH guidelines now recommend against such use outside of a clinical trial.
• Recent data from a large randomized controlled trial showed no evidence of benefit for mortality or other outcomes such as hospital length of stay or need for mechanical ventilation of HCQ treatment in hospitalized patients with COVID19.
SIGNIFICANT SIDE EFFECTS.
These studies were observational in nature, which Jha argued meant they were not of high-quality, and thus the results should be treated with caution.
"Today, the consensus in the scientific community, based on overwhelming evidence, is that hydroxychloroquine provides no benefits in treating COVID-19, and may produce significant harms," Jha said in his testimony.
Jha said that not only has the drug demonstrated "minimal to no benefit in treating COVID-19" but it also poses "substantial risks" to patients.
"Hydroxychloroquine has a very narrow therapeutic range. Only a small range of doses can be tolerated without leading to toxicity. While hydroxychloroquine toxicity is not very common, its use for COVID-19 requires a higher dosage than normally employed, and therefore, raises concern of greater side-effects and toxicity."
MY NOTE: This is a valid concern so I looked up recommended dosages and compared it to what was given in the contrarian studies. Either, the studies gave less Hydroxychloroquine that was needed to combat Covid, in other words, physicians gave beyond recommended guidelines of 600mg maximum OR a higher dosage than normally employed WASN’T given. It sure wasn’t in the studies. In any event, unless 600mg/day was exceeded, there’s no reason for heart issues to increase because of its use.
800 mg (620 mg base) followed by 400 mg (310 mg base) at 6 hours, 24 hours and 48 hours after the initial dose (total 2000 mg hydroxychloroquine sulfate or 1550 mg base).
Do not exceed 600 mg or 6.5 mg/kg (5 mg/kg base) per day, whichever is lower, as the incidence of retinopathy has been reported to be higher when this maintenance dose is exceeded.
They received 10 doses of either hydroxychloroquine or a placebo over five days (400 mg twice daily on the first day, then 200 mg twice daily for the following four days).
Earlier in the month, the FDA had revoked its emergency use authorization for hydroxychloroquine and chloroquine. It cited a lack of benefit as well as risks, such as serious heart rhythm problems.
Alam said he decided he could not apply the touted combination of the antimalarial hydroxychloroquine and antibiotic azithromycin because the side effects could be potentially fatal for his high-risk patients, many of whom had underlying heart issues.
So instead, Alam replaced azithromycin with another decades-old antibiotic that doesn’t pose any known risks to the heart.
AAPS's endorsement of the drug comes after a Veteran Affairs study of hydroxychloroquine found that those who took the drug were more likely to die, casting doubt over the potential treatment that President Trump has hailed a 'game changer.'
The group of doctors dismissed those preliminary results, claiming that the 52 people who died were very sick, meaning their outcomes are 'not indicative' of hydroxychloroquine's effects and that the drug would work better if used in patients with less critical illness.
But the Lancet paper, despite its retraction, will make it more difficult to continue current trials, White laments. Published on 22 May, the study claimed, supposedly based on data from 96,000 patients around the world, that hydroxychloroquine and chloroquine, whether given alone or in combination with another drug, caused a steep increase in deaths. That led many regulatory agencies to ask scientists to halt their trials and make sure they were not harming their patients. Recovery and Solidarity were temporarily halted but resumed after a safety committee took a look at the data.
FDA
FDA determined that chloroquine and hydroxychloroquine are unlikely to be effective in treating COVID-19 for the authorized uses in the EUA. Additionally, in light of ongoing serious cardiac adverse events and other potential serious side effects, the known and potential benefits of chloroquine and hydroxychloroquine no longer outweigh the known and potential risks for the authorized use.
Anand Shah, M.D. “The FDA always underpins its decision-making with the most trustworthy, high-quality, up-to-date evidence available.
Recent results from a large randomized clinical trial in hospitalized patients, a population similar to the population for which chloroquine and hydroxychloroquine were authorized for emergency use, demonstrated that hydroxychloroquine showed no benefit on mortality or in speeding recovery. This outcome was consistent with other new data, including data showing that the suggested dosing regimens for chloroquine and hydroxychloroquine are unlikely to kill or inhibit the virus that causes COVID-19. The totality of scientific evidence currently available indicate a lack of benefit.
This action was taken following a rigorous assessment by scientists in our Center for Drug Evaluation and Research,”
Of note, FDA approved products may be prescribed by physicians for off-label uses if they determine it is appropriate for treating their patients, including during COVID.
based on new information, including clinical trial data results, that have led BARDA to conclude that this drug may not be effective to treat COVID-19 [Coronavirus Disease 2019] and that the drug’s potential benefits for such use do not outweigh its known and potential risks.
EUA may be issued only if FDA concludes “that, based on the totality of scientific evidence available to the Secretary, including data from adequate and well-controlled clinical trials, if available, it is reasonable to believe that: (A) the product may be effective in diagnosing, treating, or preventing—(i) such disease or condition [….]; and (B) the known and potential benefits of the product, when used to diagnose, prevent, or treat such disease or condition, outweigh the known and potential risks of the product […].”
We now believe that the suggested dosing regimens for CQ and HCQ as detailed in the Fact Sheets are unlikely to produce an antiviral effect.
• Earlier observations of decreased viral shedding with HCQ or CQ treatment have not been consistently replicated and recent data from a randomized controlled trial assessing probability of negative conversion showed no difference between HCQ and standard of care alone.
• Current U.S. treatment guidelines do not recommend the use of CQ or HCQ in hospitalized patients with COVID-19 outside of a clinical trial, and the NIH guidelines now recommend against such use outside of a clinical trial.
• Recent data from a large randomized controlled trial showed no evidence of benefit for mortality or other outcomes such as hospital length of stay or need for mechanical ventilation of HCQ treatment in hospitalized patients with COVID19.
Notably, 84% of hydroxychloroquine and chloroquine cases reporting a serious cardiac adverse event also reported concomitant use of at least one other QT prolonging medication; 69% of the cases with a serious adverse cardiac event reported concomitant azithromycin use, with or without other QT prolonging medications. Fourteen cases were identified with ventricular arrhythmia, ventricular tachycardia or ventricular fibrillation; seven of these had a fatal outcome. Two of the ventricular arrhythmia cases also reported TdP, one of which was fatal.
FAERS data have limitations. First, there is no certainty that the reported event was actually due to the product. FDA does not require that a causal relationship between a product and event be proven, and reports do not always contain enough detail to properly evaluate an event. Further, FDA does not receive reports for every adverse event or medication error that occurs with a product. Many factors can influence whether or not an event will be reported, such as the time a product has been marketed and publicity about an event. Therefore, FAERS data cannot be used to calculate the incidence of an adverse event or medication error in the U.S. population.
FDA and BARDA agreed that the scientific evidence supports revocation of the EUA
News and Medical articles negative about Hydroxychloriquine
HEADLINE: Trump's praise of hydroxychloroquine led to a boom in prescriptions. Then came reports of thousands of patients experiencing adverse events.
“The benefits really didn’t outweigh the risks,” said Philip Trapskin, program director for medication use safety at UW Health. “Our thought leaders have moved on. Hydroxychloroquine is not something that we should be messing around with.”
FORBES HEADLINE: After Hydroxychloroquine, Trump Is Now Seeking To Get Another Unproven Drug Approved By The FDA: Report
“President Trump has previously pushed FDA Commissioner Stephen Hahn to approve antimalarial drug hydroxychloroquine as a cure for coronavirus, and in May announced he was taking the drug as a preventative measure. But findings in medical journal The Lancet (My note: Lancet article RETRACTED June 4 due to improper data. This article is August 17) have since found that drug is not effective against Covid-19 and can actually trigger heart arrhythmia in coronavirus patients, while the FDA, which had previously authorized the drug, has warned against the use of hydroxychloroquine and a more toxic version, chloroquine, to treat the virus because of the risk of developing “serious heart problems . . . lymph system disorders, kidney injuries, and liver problems and failure.”
Other information:
Another study
A total of 42% of the patients were receiving supplemental oxygen at baseline.
18/504 died